
Social Determinants of Health for Rural People
Social determinants of health (SDOH) are, according to Healthy People 2030,
“the conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.”
Income-level, educational attainment, race/ethnicity, and health literacy all impact the ability of people to access health services and to meet their basic needs, such as clean water and safe housing, which are essential to staying healthy. Rural residents are more likely to experience some of the contributing social factors that impact health, such as poverty. The impact of these challenges can be compounded by the barriers already present in rural areas, such as limited public transportation options and fewer choices to acquire healthy food.
This guide focuses on the barriers and challenges that rural residents experience, discussing the impact of and documenting rural differences related to:
- Income, employment, and poverty
- Educational attainment and literacy
- Race/ethnicity
- Sexual orientation/gender identity
- Health literacy
- Adequate community infrastructure, which can ensure public safety, allow access to media, and promote wellness
- Environmental health, including water quality, air quality, and pollution
- Access to safe and healthy homes, including issues related to energy costs and weatherization needs, lead-based paint, and other safety issues
- Access to safe and affordable transportation, which can impact both job access and healthcare access. Unsafe transportation, such as vehicles in poor condition, may increase risk of injury.
- Access to healthy and affordable food
- Access to healthcare services
Two related guides are available to learn about the impacts of the social determinants of health (see Rural Health Disparities) and ways to address them to improve health (see Human Services to Support Rural Healthcare).
Related Toolkits


Frequently Asked Questions
- How does Rural America differ from the nation as a whole, regarding the social determinants of health?
- What is being done to address the social determinants of health for rural residents?
- How do poverty and unemployment impact health in rural communities?
- How does early childhood development act as a social determinant? What resources are available to address this?
- How do rural areas fare on key factors impacting early childhood development?
- What are the roles of literacy, health literacy, and educational attainment in the health of rural residents?
- What types of environmental hazards do rural communities face that endanger the health of their residents?
- How does the quality of housing available in rural areas impact people's health?
- How does rural homelessness impact health?
- How can a lack of transportation options impact low-income, frail elderly, and disabled rural residents?
- How do rural residents experience food insecurity?
- What additional challenges do rural minorities face related to staying healthy?
- How do sexual orientation and gender identity impact health for rural residents?
- How do rural residents access human services that help them address social determinants of health?
- What can healthcare providers do to help address the social determinants of health for their patients?
- How can rural medical-legal partnerships help address health-harming legal needs?
- How do telephone services and broadband access impact health?
- How do the social determinants impact healthcare access for rural residents and how does healthcare access itself act as a social determinant of health for rural people?
How does Rural America differ from the nation as a whole, regarding the social determinants of health?
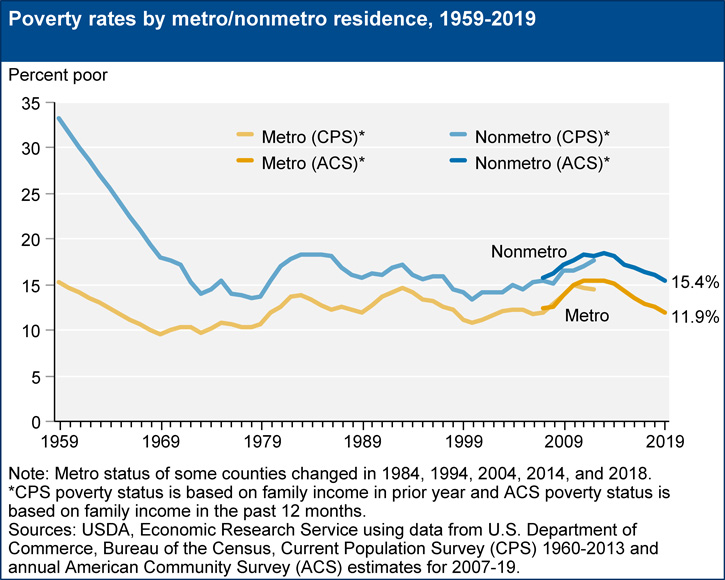
Rural America experiences many inequities compared to the nation as a whole. Often rural residents have fewer individual resources and, on average, are poorer and less educated. This Economic Research Service chart shows the ongoing gap between metropolitan and non-metro poverty rates:
Additionally, many rural residents face barriers related to access to housing, transportation, food, and water that are safe, healthy, and affordable. These barriers can impact all residents, though they are particularly problematic for those already struggling financially.
Rural communities also face many environmental challenges. Hazardous materials often end up in remote areas where the land is cheap and fewer people overall are put at risk. Rural industries like mining and farming bring with them their own dangers and environmental impacts.
The Geography of Need: Identifying Human Service Needs in Rural America, a 2011 publication from the Rural Policy Research Institute (RUPRI), identified 8 demographic and 4 economic characteristics that are indicators that a community has high human service needs. Demographic indicators included minority population, population 65 and older, veterans, adults without a high school diploma, and other factors. Economic indicators included poverty, households without vehicles, households receiving SNAP (food stamps) benefits, and income received from government transfer programs. Based on this set of 12 indicators, only 9% of metropolitan counties had three or more risk factors, while among non-metropolitan counties, 17.3% of micropolitan (large rural) and 31.2% of non-core (small rural) counties had three or more risk factors.
A 2014 article in the Annals of Internal Medicine, Neighborhood Socioeconomic Disadvantage and 30-Day Rehospitalization, examined rehospitalizations based on patients' place of residence. The study used the Area Deprivation Index (ADI – data available via the Neighborhood Atlas), a set of measures of socioeconomic deprivation such as poverty level, educational attainment, and household information, to compare neighborhoods. Patients in the study who lived in the most disadvantaged neighborhoods were at higher risk for rehospitalization, and nearly one-third of rural patients lived in such locations. One contributing factor related to rural readmissions that was not covered in this study is the lack of home health and other supportive services for discharged patients.
A variety of well-being indexes and tools share data and rankings based on factors that include social determinants of health. Some examples include:
- CDC/ATSDR Social Vulnerability Index, Agency for Toxic Substances and Disease Registry, Centers for Disease Control and Prevention (CDC)
- Multidimensional Index of Deep Disadvantage, University of Michigan
- Neighborhood Atlas, University of Wisconsin School of Medicine and Public Health
- The Opportunity Atlas, Brown University, Harvard University, U.S. Census Bureau
What is being done to address the social determinants of health for rural residents?
An ever-increasing number of federal agencies, foundations, and health-related organizations are taking an interest in the social determinants of health in general, and many are looking specifically at rural areas.
Just a few of these undertakings include:
- 2015 and 2016 meetings of the National Advisory Committee on Rural Health and Human Services in Kentucky, Minnesota, and New Mexico looked at rural poverty and the social determinants of health. The December 2015 NACRHHS policy brief, Child Poverty in Rural America, summarizes their findings from the Minnesota meeting. A January 2017 policy brief, Social Determinants of Health, summarizes their findings from the New Mexico meeting and offers policy recommendations for addressing the social determinants of health in rural communities.
- Rural Health Value, a project funded by the Federal Office of Rural Health Policy, developed a guide focused on rural providers: Understanding and Addressing Social Determinants of Health: Opportunities to Improve Health Outcomes – A Guide for Rural Health Care Leaders.
- The Association of American Medical Colleges 2016 report Achieving Health Equity: How Academic Medicine Is Addressing the Social Determinants of Health looked at both preparing physicians to meet rural needs and services for rural veterans.
- The Advisory Committee on Training in Primary Care Medicine and Dentistry's 2016 report, Addressing the Social Determinants of Health: The Role of Health Professions Education, discussed how healthcare providers can help address the social determinants of health and featured New Mexico's Health Extension Rural Office (HERO) program, which places HERO agents in rural communities to help address community health needs.
- The U.S. Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation issued December 2016 and March 2020 reports to Congress on Medicare's value-based purchasing programs that looked at a variety of social factors that impact health, including rurality.
- A February 2018 report from the NORC Walsh Center for Rural Health Analysis, Exploring Strategies to Improve Health and Equity in Rural Communities, identifies the strengths and assets of rural communities that can help address the social determinants of health.
How do poverty and unemployment impact health in rural communities?
Poverty is an ongoing problem for many rural areas. The 2014 RUPRI publication Persistent Poverty Dynamics: Understanding Poverty Trends Over 50 Years reports on counties with poverty rates above 20% over the past 50 years. Sixty-four percent of non-core (small rural) counties are persistent poverty counties, compared to 22% of micropolitan (large rural) and 14% of metropolitan counties.
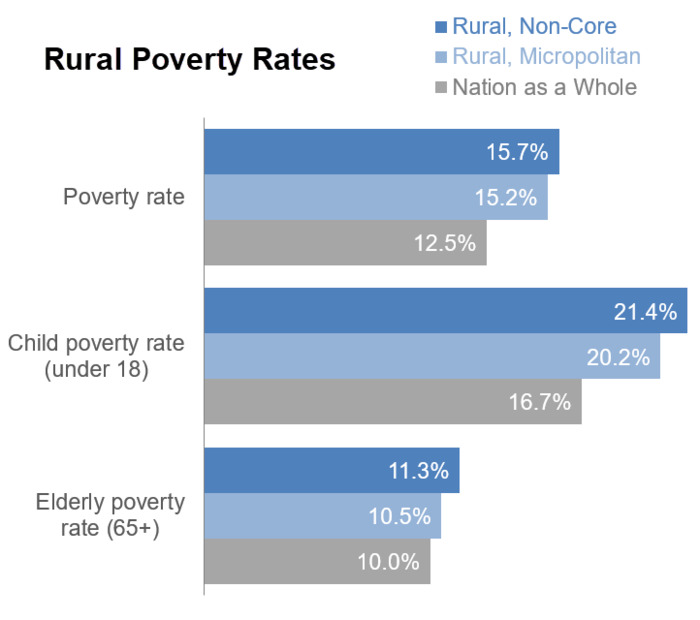
Rural areas have higher poverty rates, particularly among children and the elderly:
Average income is lower in rural areas. The nonmetro median household income in 2021 was $53,750, compared to $70,784 for the nation as a whole, as reported in the U.S. Census Bureau's Income in the United States: 2021.
A May 2016 report from the USDA Economic Research Service, Understanding the Rise in Rural Child Poverty, 2003-14, identifies factors related to the ongoing crisis of rising child poverty, including the impact of income inequality. Growing Up Rural in America, a 2018 Save the Children report, describes the impact of poverty on rural children and provides state-by-state rural child poverty data. It also addresses a number of other social determinants impacting rural children, including malnutrition, teen births, and high school drop outs.
Among the impacts of poverty on health is the barrier it creates in paying for healthcare services and meeting basic living needs, such as food and shelter, that are necessary to be healthy. Poverty also exerts an influence over health in the stress it causes. A 2012 Psychological Science article, Poverty and Health: The Mediating Role of Perceived Discrimination, reports on a longitudinal study of rural adolescents. The study looked at a range of health measures that can have long-term health consequences, such as blood pressure, cortisol levels, and body mass index. For study participants, poverty was associated with greater perceived discrimination, which in turn was associated with worse health measures.
The availability of good jobs — jobs that pay a living wage, offer adequate hours, and include benefits such as health insurance coverage and paid sick leave — can also impact rural residents' ability to stay healthy.
The 2013 Carsey Institute report Middle-Skill Jobs Remain More Common Among Rural Workers describes the continued rural reliance on mid-level jobs that require on-the-job training or apprenticeship. Urban areas tend to have a similar percentage of low-skill jobs as rural areas, fewer mid-skill jobs, and more high-skill jobs that come with bigger paychecks and benefits. In addition, workers with a college degree may find they earn less than their counterparts who work in urban areas, though those with less education may fare better in rural areas:
| Rural | Nation as a Whole | |
|---|---|---|
| All education levels | $45,851 | $48,747 |
| Less than high school graduate | $30,984 | $29,706 |
| High school graduate | $38,363 | $36,931 |
| Some college or associate's degree | $44,151 | $43,988 |
| Bachelor's degree | $59,469 | $64,982 |
| Graduate or professional degree | $75,137 | $85,680 |
| Source: Table B20004, 2018-2022 American Community Survey 5-Year Estimates | ||
A 2011 brief, also from the Carsey Institute, Rural Workers Have Less Access to Paid Sick Days, reports that 44% of rural workers lack access to paid sick leave, compared to 34% for suburban workers, and 38% for central city workers. Rural workers also fare worse in terms of paid leave to care for sick children.
How does early childhood development act as a social determinant? What resources are available to address this?
Early childhood development programs have the potential to impact health at a young age and set children on a path to growing up to be healthy adults, whatever background and resources their families have. According to Healthy People 2030,
“Early childhood development and education are key determinants of future health and well–being. Addressing the disparities in access to early childhood development and education opportunities can greatly bolster young children's future health outcomes.”
Some of the early childhood factors identified in the Improving Early Childhood Development: WHO Guideline that impact health include:
- Prenatal and delivery care
- Violence and injury prevention
- Responsive caregiving from parents and other direct caregivers
- Early learning opportunities
- Optimal nutrition for infants and young children
- Maternal mental health
How do rural areas fare on key factors impacting early childhood development?
- Health Disparities in Rural Women, from the American College of Obstetrics and Gynecologists Committee on Health Care for Underserved Women, reports on decreasing access to obstetric services in rural areas. More than half of rural women live more than 30 minutes from a hospital offering delivery and nursery services. Rural women also tend to begin prenatal care later than suburban women. A 2020 infographic from the University of Minnesota Rural Health Research Center, Loss of Hospital-based Obstetric Services in Rural Counties in the United States, 2004-2018, demonstrates that the percentage of rural counties with hospital-obstetric services decreased from 82 to 77% in micropolitan counties, and 40 to 27% in noncore counties.
-
Infant mortality is higher in nonmetropolitan counties, with a 2019 rate of 6.4 per 1,000
in nonmetro counties compared to 5.4 in metro counties:
- A 2018 Center for American Progress report, America's Child Care Deserts in 2018, found that 59% of rural communities in the United States are classified as child care deserts, or areas lacking in adequate child care center spaces for children under age five. According to a Bipartisan Policy Center (BPC) survey conducted in 2019 by Morning Consult, nearly 62% of families living in rural areas said they had difficulty finding quality child care to fit their budget; however, less than half of families living in urban areas said the same.
- Rural Head Start programs also have difficulty maintaining an adequately trained workforce of early childhood educators, according to a 2012 National Advisory Committee on Rural Health and Human Services policy brief, Challenges to Head Start and Early Childhood Development Programs in Rural Communities. They also face challenges providing the transportation necessary to get rural children to both the preschool and healthcare services required for Head Start. Some Head Start programs are home-based, and use a home visiting model to bring services directly to families, which can be an effective delivery method in rural areas.
- Rural school-age children and youth have fewer summer opportunities that support health and learning, as explained in Shaping Summertime Experiences: Opportunities to Promote Healthy Development and Well-Being for Children and Youth, a 2019 National Academies of Sciences Engineering, and Medicine consensus report.
Programs that can intervene to address early childhood development include:
- Comprehensive child wellness programs like Project LAUNCH (Linking Actions for Unmet Needs in Children's Health)
- Nutrition programs such as the USDA's Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), which provides food and nutrition education to pregnant and postpartum women, and infants and children through age 5 who would not otherwise have enough nutritious food, and the Child and Adult Care Food Program (CACFP), which helps childcare providers offer high-quality meals to children in daycare and afterschool programs.
- Home visiting programs that promote maternal and child health, child development, and positive parenting, such as those supported by HRSA's Maternal, Infant, and Early Childhood Home Visiting (MIECHV) funding.
- Programs that support full-day, full-year quality childcare, with healthy food, physical activity, appropriate learning opportunities, and role models for healthy emotional and social well-being. For example, Healthy Kids, Healthy Future provides tools for childcare and early education providers to help children develop healthy habits.
- Early childhood education programs like Head Start and Early Head Start, which help low-income families and children get ready for school through preschool education, health, and social services.
- Full-service community schools that use a model like the CDC's Whole School, Whole Community, Whole Child (WSCC) approach to help children establish healthy behaviors. For more information, see the Coalition for Community Schools.
Examples of rural projects addressing early childhood development as a social determinant include:
- Healthy Connections, Inc. Healthy Families America (HCI HFA), which provides prenatal check-ups, education, transportation, well-baby checks, and child immunizations
- MIST: Mothers and Infants Sober Together, which helps rural Tennessee mothers with substance abuse problems provide a safe, drug-free home for themselves and their newborn
- The Healthy Early Learning Project (HELP), offering physical and nutritional programs to preschools in rural Kansas
For information on how schools can support health, see RHIhub's topic guide, Rural Schools and Health.
What are the roles of literacy, health literacy, and educational attainment in the health of rural residents?
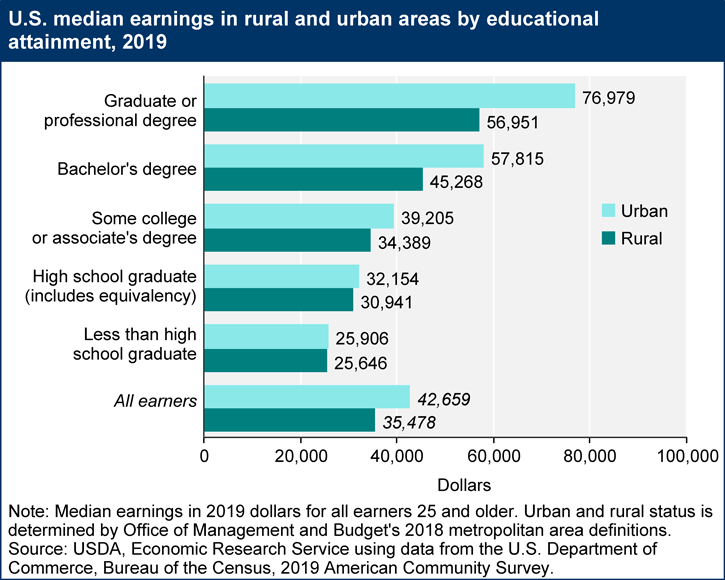
One of the most obvious impacts of educational attainment is that lower education levels impact earnings. This chart from the USDA Economic Research Service shows the relationship of education levels and median earnings for rural adults:
However, income levels are not the only impact that education has on well-being.
A 2004 article in the Journal of General Internal Medicine, Literacy and Health Outcomes: A Systematic Review of the Literature, reports on a review of 44 studies which found poorer health outcomes for those with poor reading skills. Studies reviewed linked low literacy to:
- Less likelihood of having health screenings and prevention services
- Higher risk of hospitalization
- Poorer health status
Health literacy is the degree to which patients understand basic health information such as following instructions from a healthcare provider, managing a chronic illness, or taking medication properly. Rural residents are at risk for low health literacy because they have lower educational levels as compared to residents of metropolitan areas. Low health literacy is a particular problem for people in poverty and people with limited education or English proficiency. According to the book, Health Literacy Interventions and Outcomes, limited health literacy is associated with a lower likelihood of using preventive health services, a greater likelihood of taking medicines incorrectly, and poor health status.
Learn more about how rural providers can help address health literacy in these Rural Monitor articles, which highlight health literacy tools and resources:
- A New Era of Health Literacy? Expanded Definitions, Digital Influences, and Rural Inequities
- Rural Health Literacy: Understanding Skills and Demands is Key to Improvement
- Rural Health Literacy: Who's Delivering Health Information?
Many studies have shown that educational attainment, beyond basic literacy, also impacts health. A 2006 report for the OECD's Centre for Educational Research and Innovation, Measuring the Effects of Education on Health and Civic Engagement: Proceedings of the Copenhagen Symposium, includes the chapter What Are the Effects of Education on Health? This document reviews the evidence that more years of education result in:
- Healthier behaviors
- Better health outcomes, including birth outcomes
- Higher use of preventive healthcare
- Increased life expectancy
A 2011 Population and Development Review article, The Education Effect on Population Health: A Reassessment, points out that many assume education is merely a stand-in for better socioeconomic status. The authors examined a wide range of studies that looked at education and health, and found that when socioeconomic status was controlled for, the positive impact of education persisted. A 2014 Center on Society and Health issue brief, Health Care: Necessary But Not Sufficient, reports that, for a group of patients with the same access to healthcare via coverage by the same healthcare plan and providers, those with less education had poorer health.
The role of education, literacy, and health literacy on health is critical for rural communities, where educational attainment lags behind the nation as a whole.
Rural programs to help students complete high school could have a long-term impact on the health of the rural population. Programs to help adults with low literacy improve their reading skills likewise could have health benefits for participants.
What types of environmental hazards do rural communities face that endanger the health of their residents?
Many rural areas face water quality, air quality, and other environmental challenges. Some of these problems are due to limited infrastructure to support public health, while others relate primarily to the impact of agriculture, logging, mining, and other industries on the environment.
Rebuilding the Unity of Health and the Environment in Rural America: Workshop Summary, a 2006 publication from the Institute of Medicine Roundtable on Environmental Health Sciences, Research, and Medicine, reports on environmental concerns faced by some rural communities, including:
- Exposure to pesticides, chemicals, and other toxins in ground water
- Air pollution, including dust and soil, pesticides, endotoxins, and other airborne pollutants
- Exposure to disease and animal waste for those working in animal production
Rural Water Quality
A 2015 report from the Government Accountability Office (GAO), Rural Water Infrastructure: Federal Agencies Provide Funding but Could Increase Coordination to Help Communities, reports that rural communities face challenges in paying to improve aging and outdated water and wastewater systems. These challenges result from:
- Fewer users of the water system to share the cost of major improvement projects
- Lack of technical expertise, resulting in a need to hire outside consultants to develop a project and complete the documentation required to apply for federal or state assistance
The Centers for Disease Control and Prevention's Healthy Housing Reference Manual, in Chapter 8: Rural Water Supplies and Water-Quality Issues, reports on water quality concerns for water systems not covered by the Safe Water Drinking Act. Rural households relying on well water or water from very small water systems face dangers from chemical and bacterial contamination. A 2017 Morbidity and Mortality Weekly Report article, Rural and Urban Differences in Air Quality, 2008–2012, and Community Drinking Water Quality, 2010–2015 — United States, reports that water quality decreases from urban to rural areas, based on a study of 10 contaminants.
A 2020 GAO report, Alternative Drinking Water Systems: Use by Very Small Communities, Related Cost Savings, and Technical Assistance Provided by EPA and USDA, identifies cost-effective options for communities of fewer than 10,000 people. Running Clear: Preventing Private Water Sources from Becoming a Health Hazard in Rural America, a June 2019 Rural Monitor article, describes safety concerns for private water sources and how the quality of well water can be ensured.
In addition to the infrastructure challenges, rural water quality may also be impacted by industrial pollution. The Environmental Protection Agency, in a 2015 publication Ground Water Contamination – Getting Up to Speed, identifies the following sources of contamination, all of which may impact rural water quality:
- Waste from active and abandoned mines
- Agricultural sources such as pesticides and manure
- Landfills
- Road salt
- Improperly constructed or abandoned wells
- Underground and aboveground storage tanks
Oil and natural gas production, including hydraulic fracturing (fracking), also can negatively impact rural surface-water and groundwater quality.
A free course, Groundwater and Well Care for Non-community Public Water Systems, is available to help owners and operators of non-community water systems learn the basic science of water wells and how to maintain them to ensure safe drinking water.
Rural Air Quality
Outdoor air quality is critical to everyone's health, and is particularly a concern for children, the elderly, people who have underlying health concerns, and those who are frequently outdoors, with health-related impacts of air pollution that include:
- Asthma and other breathing problems
- Pneumonia and bronchitis
- Chronic Obstructive Pulmonary Disease (COPD)
- Heart disease and stroke
- Lung cancer
Rural areas face a range of air pollutants caused by:
- Unpaved roads
- Rail transport of hazardous materials
- Pesticides
- Crop harvesting and storage
- Livestock feeding and waste
- Mining, particularly surface mining
- Oil and natural gas drilling
The National Environmental Public Health Tracking Network offers a Data Explorer Tool providing state and county-level data on outdoor air quality indicators.
Examples of rural communities working to address environmental health include:
- The Rural Desert Southwest Brownfields Coalition (RDSBC), a multi-county partnership to clean up brownfields in Nevada and California
- An environmental risk map solution used by the Navajo Nation to limit exposure to uranium in water and soil due to mine-waste contamination
The West Virginia Rural Health Research Center, which was funded by the Federal Office of Rural Health Policy from 2008-2013, undertook a number of projects related to environmental health. While the center is no longer in existence, an archive of its environmental health projects and publications is available.
How does the quality of housing available in rural areas impact people's health?
While the quality of rural housing has improved in recent decades, there are still pockets of rural America where there is a lack of affordable housing that meets the basic health needs of the population. Taking Stock: Rural People, Rural Places, Rural Housing, a 2023 report from the Housing Assistance Council (HAC), identifies several rural high poverty populations that face particular housing challenges, including farmworkers, Native Americans, and those living in the Lower Mississippi Delta, the rural Southeast, Central Appalachia, or in colonias on the U.S.-Mexico border. According to the report, 5.6% of homes in rural areas of the U.S. are considered inadequate in quality.
Some of the key housing concerns that impact health include:
- Plumbing and wastewater systems (or lack thereof), which can impact water quality and contribute to illness.
- Heating and cooling methods, which impact indoor air quality and safety, for example through the use of kerosene heaters.
- Lack of smoke alarms, carbon dioxide, and carbon monoxide detectors.
- Weatherization needs and energy costs, which impact whether a house can be maintained at a temperature healthy to its inhabitants.
- Safety concerns such as lead-based paint, mold, and pests.
- Overcrowding, which can spread communicable disease and also negatively influences issues such as substance abuse and domestic violence.
HAC's Taking Stock report identifies a number of concerns related to rural housing quality:
- More than 30% of the nation's housing lacking plumbing are in rural areas, with this burden falling disproportionately on those living in colonias on the U.S.-Mexico border, on Native American lands, in Central Appalachia, the Lower Mississippi Delta, and the rural Southeast.
- Overcrowding is a problem among some low-income rural populations such as farmworkers and can have a particularly negative impact on the well-being of children.
- Rural racial and ethnic minority populations are more likely to live in substandard housing.
- Rural renters are more likely to live in substandard housing and to experience multiple housing problems related to affordability, quality deficiencies, and crowding, compared to rural homeowners.
A 2006 report from the Centers for Disease Control and Prevention, the Healthy Housing Reference Manual, reports on other concerns facing some rural residents:
- Drinking water from sources not covered by the Safe Water Drinking Act
- Reliance on septic tank systems to treat wastewater, which can result in contamination of the water supply
- Use of fuel-fired heat sources, such as coal, fireplaces, and wood stoves, which put rural residents at risk for fires. These types of heat sources, if not properly vented, may result in poor indoor air quality.
For examples of programs to help address rural housing concerns, see What are some rural housing and weatherization programs? on RHIhub's Human Services to Support Rural Health topic guide.
The Rural Monitor article Exploring the Intersection of Rural Housing Quality and Health: Healthcare Providers and Housing Experts Provide Insight discusses the impact of rural housing quality on health, as well as how public health and healthcare organizations can work with human services and housing organizations to improve the health and well-being of their community’s residents.
How does rural homelessness impact health?
Rural homeless families and individuals face a variety of challenges accessing healthcare. The lack of a stable address can make it difficult to enroll in programs they are eligible for, such as Medicaid. Even when coverage is obtained, rural people who are experiencing homelessness may face challenges finding a healthcare provider. Many need help with mental health and substance abuse problems, and the availability of these services is often limited in rural areas.
Homelessness in Rural America, a 2014 policy brief from the National Advisory Committee on Rural Health and Human Services (NACRHHS), offers an overview of how homelessness impacts rural people. Families with children are a bigger proportion of the homeless population in rural areas, compared to urban areas. A 2019 report from the Institute for Children, Poverty & Homeless, Student Homelessness in Rural America, reports that homelessness among rural public school children is growing at four times the national rate, with an increase of 11% from the 2013-2014 school year to the 2016-2017 school year. The children in families experiencing homelessness are at risk for a range of health-related consequences. According to a 2012 Child Trends publication, When the Bough Breaks: The Effects of Homelessness on Young Children, children who have unstable housing are more likely to experience:
- Emotional and behavioral problems
- Negative impacts on their physical, emotional and cognitive development
- Hunger
- Missed educational opportunities and poorer academic performance
- Acute and chronic health problems
- Exposure to violence
The NACRHHS brief describes the nature of rural homelessness and the barriers faced by the homeless in rural areas. Rural homeless people are more likely to live in substandard housing, in vehicles, or doubled up with family or friends, rather than on the street. The barriers to addressing rural homelessness include:
- Difficulty finding transportation to reach services
- A sense of isolation
- Lack of homeless-specific services in their community
- Funding programs that lack the flexibility to meet the particular needs of rural areas
- Lack of employment opportunities to help people become self-sustaining
- Difficulty applying for services, either due to lack of a permanent address or lack of Internet access
- Shortages of affordable housing
Since 2010 Pathways Vermont has addressed the homelessness challenge by using an evidence-based, cost-effective housing model, the rural-focused Housing First Program, that offers a rapid re-housing program and support services to individuals with mental health and substance use conditions. Pathways also partners with state and community organizations to expand their reach to other populations including families at-risk, veterans, and incarcerated individuals transitioning into society to offset the negative effect of prolonged exposure to homelessness. The Rural Monitor article, Looking at the Rural Homelessness Experience: Definitions, Data, and Solutions, reports on how this approach is helping the state's rural homeless population. The Rural Monitor also features other programs aimed at addressing rural homelessness.
How can a lack of transportation options impact low-income, frail elderly, and disabled rural residents?
People living in rural areas tend to be dependent on cars for transportation. These regions often lack the types of public transportation available in more populous areas. Even if there is some form of bus service, it is less likely to run at convenient times for getting to a job, taking children to daycare, or accessing needed healthcare. Of workers 16 and over who live in rural areas, only 0.36% traveled to work by public (non-taxi) transportation, compared to 3.77% for the U.S. as a whole, based on 2018-2022 American Community Survey data (Table B08141).
Low-income rural residents who are fortunate enough to own a vehicle may find the costs of gas and maintenance make it difficult to maintain reliable transportation. Poor rural residents' vehicles are often older and unreliable, and rural drivers are likely to be driving longer distances on secondary roads. Depending on the region, weather and industry may also impact road safety. These factors contribute to the higher risk of traffic injury and death for rural residents.
For those who are not able to drive due to physical limitations, lack of transportation options in rural areas can make it difficult to get to the grocery store and pharmacy, take advantage of social interactions that support good mental health, and access healthcare services.
For more information on the impact of transportation on health, see RHIhub's Transportation to Support Rural Healthcare guide.
How do rural residents experience food insecurity?
Many rural residents have fewer choices to buy fresh and affordable food, making it difficult for them to purchase the nutritious food needed to stay healthy. For those on limited incomes and with limited transportation options, it is even more difficult to meet nutritional needs. According to the USDA Economic Research Service report, Household Food Security in the United States in 2022, 14.7% of rural households are food insecure — lacking access to sufficient food — compared to 12.8% for the nation as a whole. Households with children are impacted even more, with 19.7% of rural households with children being food insecure, compared to 17.3% overall.
Food insecurity is also related to obesity, and obesity levels in rural areas tend to be higher. Rural Healthy People 2020: A Companion Document to Healthy People 2020, Volume 1 looks at rural food insecurity, obesity, and related health problems in the chapter "Nutrition and Weight Status in Rural Areas."
For an in-depth examination of these issues, see RHIhub's Rural Hunger and Access to Healthy Food and Rural Obesity and Weight Control topic guides.
What additional challenges do rural racial and ethnic minority populations face related to staying healthy?
This 2019 series of policy briefs from the Rural & Minority Health Research Center looks at social determinants of health for specific rural racial and ethnic minority populations. Each brief provides socioeconomic data, information on types of rural communities where these populations are concentrated, access to healthcare services, risk factors, and more:
- Social Determinants of Health among Rural American Indian and Alaska Native Populations
- Social Determinants of Health among Rural Asian and Pacific Islander Populations
- Social Determinants of Health among the Rural African American Population
- Social Determinants of Health among the Rural Hispanic Population
Many rural minorities face discrimination and racism that can result in stress, negatively impacting their health. Unfair treatment may impact rural minorities' ability to fully access services to support health, including healthcare services.
A 2020 Health Affairs article, Discrimination: A Social Determinant of Health Inequities discusses discrimination as a social determinant of health and its contribution to health inequities in people and communities of color. Research noted that discrimination impacts health in 3 major ways: psychosocial stress, access to health and social services, and violence and bodily harm, which may interact with one another. Discrimination can result in:
- Severe stress, anxiety, or depression
- Alcohol and substance abuse
- Overall poor cardiovascular and metabolic health
- Sleep disturbances
- Limited access to health and social resources
- Discriminatory violence
Cultural beliefs can also act as a social determinant. A belief might undermine health. For example, not expecting a long lifespan may result in life choices that don't support health. Cultural beliefs may also serve as barriers to connecting with healthcare providers.
Culture as a Social Determinant of Health, a 2012 paper commissioned by the Institute of Medicine's Roundtable on the Promotion of Health Equity and the Elimination of Health Disparities, discusses how a healthcare system that doesn't respect the beliefs and culture of Native American patients may result in patient experiences that include:
- Patients not following healthcare providers' advice and instructions
- Reluctance to use the healthcare system
- An experience of alienation, fear, and disrespect
Healthcare providers, in turn, may misunderstand their patients, assuming they are not interested in their own health or not able to follow instructions. The development of cultural competence is a key method for healthcare providers to help better address the needs of minority populations.
Examples of rural communities working to address these challenges include:
- The Conetoe Family Life Center and its founder, Reverend Richard Joyner, who work to improve population health in a predominately African-American community, as featured in the Rural Monitor June 2016 article, The Reverend's Revolution: A Kid-First Approach to Community Health.
- The Health without Borders program, which brings a door-to-door immunization approach common in Mexico to a largely Hispanic/Latino population in rural New Mexico.
- Good Health and Wellness in Indian Country, a CDC initiative supporting tribes and tribal organizations implementing culturally adapted, community-selected strategies to address health literacy, nutrition, physical activity, and more.
For more project examples, see Rural Health Models & Innovations by Topic: Racial and ethnic groups.
How do sexual orientation and gender identity impact health for rural residents?
Rural lesbian, gay, bisexual, transgender, questioning/queer, and intersex (LGBTQI+) residents face a range of challenges to staying healthy related to their sexual orientation and gender identity. A May 2016 Rural Monitor article, LGBTQ Healthcare: Building Inclusive Rural Practices, describes some of the barriers to healthcare that rural LGBTQ+ people face, including:
- Not accessing healthcare due to anticipated, internalized, and enacted stigma
- Privacy and confidentiality concerns
- Patients not disclosing sexual orientation or gender identity to a provider, which could impact provision of needed urgent and preventive care
- Limited training of healthcare providers related to LGBTQ+ health-related issues
- Provider bias or discrimination, which can be more problematic in a rural area with fewer providers to choose from
Addressing the Social Determinants of Health Inequities Among Gay Men and Other Men Who Have Sex with Men in the United States, a 2014 report from Trust for America's Health, points out additional factors that impact health for the LGBTQ+ population:
- Higher poverty rates
- For LGBTQ+ youth, family rejection and homelessness
- More likely to receive punishment from schools, police, and the court system
- Higher rates of psychiatric disorders and suicide related to stigma and discrimination
- Being the target of violence, abuse, and bullying
- For those living with HIV, additional stigma related to their infection
The 2016 Rural Monitor article identifies resources and approaches rural providers can adapt to help meet the healthcare needs of their LGBTQ+ patients. In addition, a 2016 Journal of the American Board of Family Medicine article, Stakeholders' Recommendations to Improve Patient-centered “LGBTQ” Primary Care in Rural and Multicultural Practices, offers guidance to primary care providers to improve care delivery for this population.
How do rural residents access human services that help them address social determinants of health?
A range of federal and state programs address human needs, from income supports to job training to housing assistance and more. For detailed information on services available in rural communities:
- Human Services to Support Rural Healthcare
- Rural Hunger and Access to Healthy Food
- Transportation to Support Rural Healthcare
The NACRHHS policy brief, The Intersection of Rural Poverty and Federal Human Services Programs, features case studies of two communities using strategies to integrate services to make it easier for people experiencing poverty to access the range of services they need. RHIhub's Rural Services Integration Toolkit is a guide to developing programs that integrate rural health and human services to better meet rural residents' needs. The toolkit identifies 9 programs in a variety of settings and regions that are taking different approaches to services integration.
State human service agencies provide varying degrees of access to services and to assistance programs via online portals. When available, together with adequate broadband service and other necessary infrastructure, access to human services is faster and easier. Some agencies also offer mobile van services to rural residents, although these tend to be confined to specific populations such as migrant workers.
What can healthcare providers do to help address the social determinants of health for their patients?
An April 2018 Rural Monitor article, Social Determinants of Health: Transforming the Buzz Phrase to a Rural Action Item, looks at the social determinants from a provider's perspective, discussing what rural healthcare facilities can do to help their patients:
- Tift Regional Health System in rural Georgia conducts social risk assessments for clinic and hospital patients, with support from the CMS Innovation Center's Accountable Health Communities Model.
- CommWell Health's NC-Rurally Engaging and Assisting Clients who are HIV positive and Homeless (NC-REACH) works with community service organizations in rural North Carolina to address housing needs identified through their social determinant risk screening process.
The American Hospital Association (AHA), in an invited commentary in the September 2018 issue of Academic Medicine — Ensuring Access to Quality Health Care in Vulnerable Communities — identifies “addressing social determinants of health” as an important strategy for hospitals. Providers can screen for health-related social needs, help patients access community services, and align local services with patient needs. AHA offers a collection of guides to help hospitals address food, housing, and other social determinants of health in their communities:
The Agency for Healthcare Research and Quality offers a guide to help primary care practices collect social needs information from patients and connect them to relevant community resources:
The American Academy of Family Physicians's EveryONE Project provides tools for physicians and practice teams to help address the social determinants of health:
- The EveryONE Project Toolkit includes a variety of tools for social needs screening and action plan development, as well as information on building a culture of health equity.
- Addressing Social Determinants of Health in Primary Care: Team-based Approach for Advancing Health Equity is an implementation guide for practice teams focused on developing a culture of health equity and a team-based approach to addressing the social determinants.
Healthcare providers and health systems may want to consult the Commonwealth Fund’s Return on Investment (ROI) Calculator for Partnerships to Address the Social Determinants of Health when considering interventions to address the social determinants of health. It can help organizations plan sustainable financial arrangements, with a focus on addressing the needs of high-need, high-cost patients.
Community health needs assessments (CHNAs) can help healthcare organizations determine which social determinants of health would be most impactful to address in their communities. For more on needs assessments, see RHIhub's Conducting Rural Health Research, Needs Assessment, and Program Evaluation.
How can rural medical-legal partnerships help address health-harming legal needs?
An April 2022 study from the Legal Services Corporation, The Justice Gap: The Unmet Civil Legal Needs of Low-income Americans, reports on legal needs related to healthcare access, the impact of COVID-19 on American families, and other issues that influence health, such as housing and poverty. It includes an infographic highlighting the prevalence of civil legal problems and the need for legal help for people in rural areas.
Medical-legal partnerships help healthcare providers and lawyers work together in addressing patients' health-harming legal needs. The National Center for Medical-Legal Partnership's How Legal Services Help Health Care Address Social Needs, identifies the following issues where legal aid interventions can help:
- Appealing denial of benefits, such as health insurance, disability benefits, and food stamps
- Addressing housing quality, housing subsidies, and access to utilities
- Protecting workers from discrimination
- Helping veterans with discharge status
- Managing family law concerns related to domestic violence, custody, and other issues
Bringing Law and Medicine Together to Help Rural Patients, an October 2016 Rural Monitor article, highlights rural medical-legal partnerships, and discusses the benefits MLPs bring to rural patients, including:
- Reduced stress levels
- Greater patient engagement
- Improved health outcomes
FirstHealth of the Carolinas, in response to findings from a community health needs assessment, established an MLP in rural North Carolina in partnership with Legal Aid of North Carolina, Inc. Their work is featured in a 2017 Rural Health Value profile, Medical-Legal Partnership Addresses Social Determinants of Health.
How do telephone services and broadband access impact health?
Access to basic telephone service and smartphone technology helps ensure that rural residents can:
- Make appointments with healthcare providers and other service providers
- Contact emergency medical services
- Receive health coaching and other disease management services available by phone
- Stay in touch with family and friends, which may allow rural older adults to stay independent longer
Connectivity now plays a much greater role in healthcare, with broadband access offering the potential for rural residents to:
- Learn about health topics online
- Access their electronic health records
- Participate in home monitoring and other telehealth services
- Have face-to-face connections to distant family and friends
- Learn about and access government programs
Despite the promise of this technology, not all families are in a position to take advantage of these opportunities. According to the Pew Research Center's August 2021 article, Digital Gap Between Rural and Nonrural America Persists, only 72% of rural households have home broadband access, compared to 77% of urban and 79% of suburban households. Mapping Broadband Health in America, a visualization tool from the Federal Communications Commission (FCC), shows broadband access as it relates to health factors and demographics and includes rural data.
In many rural communities, the local library provides access to public computers and the internet, as well as training on how to search for health and other information. Rural Libraries in the United States: Recent Strides, Future, Possibilities, and Meeting Community Needs, a 2017 report from the American Library Association, documents the availability of different services, finding that rural libraries typically offer slower broadband than their urban counterparts but are just as likely as urban libraries to provide public Wi-Fi.
The Federal Communications Commission's Lifeline Program can help make telephone service more affordable for low-income people. To better meet the expanding need for connectivity, in March 2016 the program was expanded to also support discounted broadband for those who qualify. The FCC's Connect America Fund (CAF) aims to accelerate infrastructure development by subsidizing telephone companies to add broadband service where it is not yet available, including rural areas. Connecting Americans to Health Care is an FCC initiative supporting telehealth focused on the potential of remote patient monitoring and mobile health applications to help rural patients.
How do the social determinants impact healthcare access for rural residents and how does healthcare access itself act as a social determinant of health for rural people?
Social determinants that impact access to healthcare include:
- Poverty, income, and employment status, all of which contribute to whether an individual has:
- Health insurance coverage, whether through an employer, a public program, or their own purchase
- The ability to pay out-of-pocket costs such as co-pays and prescription drug costs
- Access to dental care, either through dental insurance or the ability to pay for treatment
- Time off work to go to an appointment
- A means of transportation to visit a healthcare provider
- Resources to afford retirement and pay for healthcare and health-related expenses in retirement, including costs related to aging in place
- The health literacy skills to effectively communicate with healthcare providers and self-manage their care.
Healthcare access can itself act as a social determinant for rural residents. Living in a rural community that has limited health services available is an added barrier to achieving good health. The burden may be a lack of a specific kind of service, such as dental or behavioral health services, or may be related to the hours that a service is available, for example weekends and evenings. A June 2016 issue brief, Impacts of the Affordable Care Act's Medicaid Expansion on Insurance Coverage and Access to Care, found that increased healthcare access through Medicaid expansion improved individuals' financial well-being.
Certain public health services, which support population health, may also be less available in rural communities. For example, rural residents have less access to fluoridated water. While this is partly because they are more likely to be on well water, rural water systems are also less likely to be fluoridated. For more information on fluoridation, see Where can I find information about fluoridation in rural community water supplies? on RHIhub's Oral Health in Rural Communities topic guide. For additional information on rural public health services, see RHIhub's Rural Public Health Agencies topic guide.
A lack of healthcare and public health access may also deter businesses from locating in or expanding in a rural community, meaning fewer jobs that could lift rural residents up and make it easier for them to achieve good health. A 2006 Health Services Research article, The Effect of Rural Hospital Closures on Community Economic Health, reports that communities where the sole hospital closed saw both a reduction in per capita income and an increase in unemployment.
For a more in-depth discussion of healthcare access, see RHIhub's Healthcare Access in Rural Communities topic guide.