
Rural Hospice and Palliative Care
Hospice and palliative care services can improve the quality of life for rural residents of all ages who are dealing with serious illness or injury.
Hospice provides care to people experiencing terminal illness with a life expectancy of six months or less if the disease runs its natural course. It is based on the belief that everyone has the right to die pain-free and with dignity. The focus is on compassion, caring, and quality of life, not curing. It helps patients and their families live life to its fullest.
Palliative care — also called comfort care, supportive care, or symptom management — is specialized care that treats the symptoms or suffering related to an illness at any stage of the diagnosis. It can be integrated into any healthcare setting and is delivered by a team of healthcare professionals with support from a palliative care specialist, if available. Palliative care is associated with better quality of life, improved symptom management, and higher patient satisfaction. Although palliative care is a key component of hospice care, palliative care is not restricted to patients with terminal conditions. Palliative Care or Hospice Care? compares these services.
According to the National Advisory Committee on Rural Health and Human Services' Rural Implications of Changes to the Medicare Hospice Benefit and Stratis Health's Rural Community-Based Palliative Care: Final Report, rural residents may have limited access to hospice and palliative care. This is especially problematic since rural people tend to be older, sicker, and have lower incomes than their urban counterparts.
Use of hospice services by Medicare beneficiaries has increased since 2000 in all location types, but hospice is still used most often in urban areas.
| 2010 | 2022 | |
|---|---|---|
| Urban | 45.6 | 50.2 |
| Micropolitan | 39.2 | 47.2 |
| Rural, adjacent to urban | 39.0 | 47.8 |
| Rural, nonadjacent | 33.8 | 42.1 |
| Frontier | 29.2 | 35.2 |
| Source: Table 9-2, Report to Congress: Medicare Payment Policy: Hospice Services, MedPAC, March 2024. | ||
According to the Hospice services chapter in the March 2024 Report to the Congress: Medicare Payment Policy, as of 2022 there were 827 rural hospices, down from 871 in 2018. The report notes that although the number of rural hospices decreased, the percentage of rural Medicare decedents using hospice services increased over this period. In 2022, about 14% of hospices in the United States were located in rural areas.
Frequently Asked Questions
- What types of services do hospice and palliative care provide?
- How are hospice and palliative care providers reimbursed for their services?
- Who offers hospice and palliative care in rural areas and in what settings are they provided?
- Who is included in rural hospice and palliative care teams?
- How can palliative care be used in rural communities to improve the quality of life of people dealing with serious illness?
- What challenges are faced by rural palliative care organizations?
- What challenges are faced by rural hospice organizations?
- What challenges are faced by the rural hospice and palliative care workforce?
- How do rural hospices utilize volunteers?
- What strategies can help make a rural hospice service financially viable?
- What strategies can help make a rural palliative care service financially viable?
- How do rural hospice providers compare on quality of care and patient satisfaction measures?
What types of services do hospice and palliative care provide?
Hospice is designed to provide care for people who are likely to die within six months, if their disease progresses at its expected pace. It provides medical, emotional, and spiritual comfort.
According to the MLN publication Creating an Effective Hospice Plan of Care, all CMS-certified hospice agencies must provide and follow an individualized plan of care for each patient. The plan of care must include all services to palliate and manage the terminal illness and related conditions of the patient. These services may include some or all of the following, depending on the patient's condition:
- Medical care provided by doctors, physician assistants, and nurses
- Medications for pain relief or symptom management
- Social work services
- Dietary counseling
- Physical, occupational, and speech-language therapy (including help with swallowing)
- Grief and bereavement counseling for the patient and family members
- Spiritual counseling
- Medical supplies and equipment related to the patient's diagnosis
- Hospice aide and homemaker services
- Goals of care discussions
A member of the hospice team can be reached at all times to answer questions and to visit patients when needed. Intermittent nursing visits are scheduled to assess and monitor patients' conditions and treat symptoms. This can include giving injections and setting up IV medication. Hospice professionals and volunteers can also teach caregivers and family members ways to help their loved one.
Patients whose conditions improve can choose to suspend hospice care and may resume services later on, if they wish. Re-election of hospice benefits is allowed by Medicare, Medicaid, and most insurance companies. Hospice also offers bereavement services for family members and caregivers for up to one year following the patient's death.
While palliative care is an important component of hospice care, it is also provided to patients who have advanced chronic diseases and other serious illnesses but are not necessarily expected to die within a few months. A terminal prognosis is not required to receive palliative care. For example, a chronic obstructive pulmonary disease (COPD) patient may receive palliative care to manage anxiety, discomfort, or insomnia related to breathing difficulty. According to the Center to Advance Palliative Care's document Serious Illness Strategies for Health Plans and Accountable Care Organizations, effective palliative care should:
- Identify the right population needing palliative care, and adjust services as patients' needs change
- Provide expert management of pain and symptoms
- Help patients and their families with decision-making regarding treatment and services
- Support family caregivers through education, counseling, and respite care
- Provide timely and appropriate care night or day to avoid unnecessary 911 calls, emergency department visits, hospitalizations, and intensive care
Core values of both hospice and palliative care include:
- Patient- and family-centered care
- Holistic relief of physical, emotional, and spiritual suffering
- Interdisciplinary case management
- Ethical behavior
- Service excellence
How are hospice and palliative care providers reimbursed for their services?
Medicare pays hospice providers a daily rate for all services regardless of the services provided each day. Typically, there is no out-of-pocket cost for a patient receiving hospice care. The hospice provider assumes responsibility for all care related to the patient's terminal diagnosis and related conditions. Medicare reimburses hospice providers for four different levels of care to meet the needs of patients:
- Routine home care – the most common level of care provided, accounting for 98% of hospice care in 2019. Routine home care is reimbursed at one rate for the first 60 days of care, and a lower rate for every subsequent day of care.
- Continuous home care – home-based care for a short-term symptom crisis that requires eight hours of care or more per day.
- Inpatient respite care – care provided in a facility setting for up to five days to provide respite for an informal caregiver.
- General inpatient care – short-term inpatient care to manage symptoms that cannot be managed in another setting.
The level of care a patient receives can change throughout their time on hospice care.
Although most states have a hospice benefit as part of their Medicaid programs, states are not required to include hospice as part of Medicaid. Medicaid hospice reimbursement is based on the Medicare hospice reimbursement rates.
Traditionally, when a patient enrolled in Medicaid Advantage (MA) elects to receive hospice care, traditional fee-for-service Medicare becomes financially responsible for hospice care and most other Medicare services, while the MA plan retains coverage of supplemental benefits. Beginning January 1, 2021, the Centers for Medicare and Medicaid Services (CMS) began to test the Hospice Benefit Component of the Value-Based Insurance Design (VBID) Model. Participating Medicare Advantage plans will be responsible for all traditional Medicare services, including hospice care.
According to the 2020 NHPCO Palliative Care Needs Survey, Medicare Part B was the most common source of palliative care reimbursement. Unlike hospice care, however, there is currently not a specific Medicare benefit for palliative care. Instead, Sustainability Strategies for Community-based Palliative Care explains that palliative care teams can often bill traditional Medicare for advance care planning and care management services. Licensed clinical social workers may also be reimbursed for mental health services provided to patients receiving palliative care services in some situations. As a result, patients experience variation in access to palliative care services. Patients may also be responsible for a copayment for these services. Palliative care programs also receive reimbursement from contracts with commercial payers, hospitals or other partnerships, philanthropies and grants, the Medicare home health benefit, and arrangements with Accountable Care Organizations and Medicare Shared Savings Plans.
Who offers hospice and palliative care in rural areas and in what settings are they provided?
According to Providing Hospice and Palliative Care in Rural and Frontier Areas, rural hospice and palliative care can be:
- Community-based
- Hospital-based
- Home health agency-based
- County health department sponsored
Community-based hospice and palliative care is the most familiar model in rural areas and is usually organized by health professionals and volunteers. These providers may serve one or more rural areas. Hospice care is typically provided in a patient's home, including an assisted living facility or nursing home, but it can also be provided in an inpatient facility.
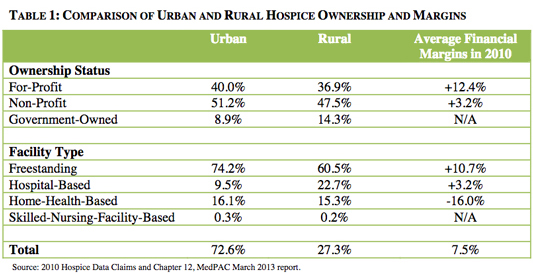
Rural Implications of Changes to the Medicare Hospice Benefit compares rural and urban hospice ownership status and facility type (see Table 1 below). In rural areas, there are more government-owned hospices, more hospital-based facilities, and fewer freestanding hospices. The report states that hospital-based hospice facilities are more prevalent in rural areas than in urban, which may be due to hospitals in many rural areas being the only source of healthcare.
Additional hospice services may be provided in hospitals, nursing homes, long-term care facilities, and private hospice centers. According to The Financial Importance of Medicare Post-Acute and Hospice Care to Rural Hospitals, 131 Critical Access Hospitals and 156 rural Prospective Payment System Hospitals reported Medicare Cost Reports for hospice services in 2015.
America's Care of Serious Illness: A State-by-State Report Card on Access to Palliative Care in Our Nation's Hospitals, a 2019 publication by the Center to Advance Palliative Care and the National Palliative Care Research Center, notes that while 71.5% of hospitals with more than 50 beds have a palliative care program, only 40% of sole community providers and 36.3% of hospitals with fewer than 50 beds have similar programs.
Who is included in rural hospice and palliative care teams?
Hospice and palliative care are provided by interdisciplinary teams that help patients approach the end of life with comfort, peace, and dignity.
Hospice teams often include, but are not limited to:
- Physicians
- Nurses
- Therapists
- Home health aides
- Bereavement and spiritual counselors
- Social workers
- Volunteers
The patient and his or her family are considered part of the hospice team, as well.
Physicians, nurse practitioners, and physician assistants are recognized by Medicare as designated hospice attending providers, though nurse practitioners and physician assistants have restrictions regarding certifying a terminal illness and conducting face-to-face encounters. Clinical nurse specialists and outside attending physicians cannot be attending providers, nor are they authorized to perform face-to-face encounters. These meetings are required before the first 180 days and every 60 days thereafter. For rural hospice programs that may not have a physician or nurse practitioner available at all times, these requirements can be difficult to fulfill. After patients have been admitted to a hospice program, the interdisciplinary team formulates a written plan of care.
The Consolidated Appropriations Act, 2021, included a provision formerly known as the “Rural Access to Hospice Act.” Beginning January 1, 2022, physicians, nurse practitioners, and physician assistants at Rural Health Clinics (RHCs) and Federally Qualified Health Centers (FQHCs) will be able to serve as attending providers for hospice patients. Historically, physicians employed by RHCs and FQHCs were unable to serve as attending physicians because RHCs and FQHCs are paid a fixed all-inclusive payment for all services to Medicare beneficiaries.
How can palliative care be used in rural communities to improve the quality of life of people dealing with serious illness?
Rural populations tend to be older and experience higher rates of disability and chronic disease than urban populations. Due to the shortage of healthcare professionals in many rural areas, rural residents may not be able to easily access their providers to address emerging or worsening symptoms of an illness. Palliative care teams can support these patients to alleviate not only the physical effects of their condition, but the emotional, social, and spiritual effects as well. Sustainability Strategies for Community-based Palliative Care also highlights that palliative care services can allow patients to continue to receive care in their communities.
What challenges are faced by rural palliative care organizations?
The 2020 NHPCO Palliative Care Needs Survey documents that palliative care providers face challenges like those experienced by hospice care providers. Respondents identified referrals, reimbursement, and staffing among their greatest challenges or barriers to providing palliative care services. Rural Community-Based Palliative Care: Final Report notes that there is a projected shortage of hospice and palliative medicine providers, and that rural areas are expected to see the greatest shortages.
Palliative care programs also experience their own unique challenges. As noted in the Rural Monitor article Community-based Palliative Care: Scaling Access for Rural Populations, medical professionals as well as lay people sometimes confuse palliative care with hospice care, and mistakenly assume that palliative treatment is appropriate only for people who are nearing the end of life. The same article notes that although hospice care is covered by many insurance plans as a benefit, palliative care typically is not.
What challenges are faced by rural hospice organizations?
Providing hospice and palliative care in rural areas involves challenges such as shortages of family caregivers, financial reimbursement problems, lack of qualified staff, and travel distances.
The policy brief, Perspectives of Rural Hospice Directors, presents the results of a 2013 phone survey of 53 rural hospice directors and key staff from 47 states. The most important issues identified by these hospice directors were:
- Financial issues, such as reimbursement and operating costs
- Rural factors, including population change, economics, culture, and geography
- Stringent federal regulations and policies, such as the requirement for face-to-face visits for recertification of hospice patients
- Workforce issues, including challenges in recruiting and retaining staff, and staff burnout
- Relationships with other health providers, and competition for resources and patients
- Technology issues, including limited access to broadband and connectivity problems
What challenges are faced by the rural hospice and palliative care workforce?
Perspectives of Rural Hospice Directors identifies heavy workloads, wearing multiple hats, and limited options for training as challenges for the rural hospice workforce. Other challenges for the rural hospice and palliative care workforce can include:
- Coping with fear and anger among patients and families who are having difficulty accepting the patients' illness or injury
- Emotional stress of caring for dying patients with whom they have close relationships
- Safety concerns related to traveling to remote areas with poor roads and communication infrastructure
- Lack of training programs geared specifically toward medical professionals who wish to specialize in hospice and palliative care
- Low retention rate among rural hospice staff
- Physical stress related to lifting heavy weights
- Salaries that may be lower than those earned by medical professionals in other specialty areas
- Work in some cases may be only part-time
- Skill set for a variety of complex chronic conditions may be required
- Scheduling such that hospice and palliative care providers may routinely work alone and without support
- Fewer medications and less medical equipment available in rural pharmacies
How do rural hospices utilize volunteers?
According to the National Hospice and Palliative Care Organization's Facts and Figures, hospice is the only Medicare provider type with Conditions of Participation that require at least 5% of patient care hours to be provided by volunteers. These community members offer a valuable service to rural hospice and palliative care agencies when they provide direct patient care, clinical support, and other general supportive services to supplement the work of hospice professionals.
As stated in Providing Hospice and Palliative Care in Rural and Frontier Areas, rural hospice and palliative care volunteers perform a variety of duties, such as:
- Visiting patients and their families, providing comfort, and preserving dignity
- Providing respite care to family members
- Grocery shopping, house cleaning, running errands, and providing rides to medical appointments
- Supporting hospice and palliative care programs by doing routine office work and participating in fundraising and marketing
Most hospice programs have an application and interview process for screening volunteers, and training programs for those who are accepted. Topics can include:
- Confidentiality issues
- Listening skills
- Signs and symptoms of impending death
- Grief support for families
Challenges in volunteer management may include:
- The need for ongoing recruitment efforts, given the small pool of potential volunteers in rural communities
- Providing adequate emotional and bereavement support for volunteers
- Providing training programs
- The aging of the volunteer workforce in rural areas
- Transportation problems, including travel over long distances or difficult terrain, and use of volunteers who might not have valid driver's licenses
- Maintaining patient confidentiality in locations where most community members are acquainted with each other
- Showing adequate appreciation for volunteers
- Meeting the CMS requirement that hospices have at least 5% of their direct patient care hours provided by volunteers
What strategies can help make a rural hospice service financially viable?
According to Perspectives of Rural Hospice Directors, rural hospices and palliative care programs face financial challenges, which can be acute and hard to resolve. These include:
- Inadequate Medicare reimbursement
- Costs associated with travel
- Regulatory requirements with financial implications
- Higher costs due to greater numbers of direct care encounters by providers treating patients at home
- Smaller number of freestanding or for-profit rural hospices
- Shorter average length of stay
- Operating costs that are not included in the per diem rate
As stated in Rural Implications of Changes to the Medicare Hospice Benefit, rural hospices face barriers in providing service. These barriers can make it difficult for rural communities to maintain Medicare-certified hospice programs, and may include:
- Low patient volume, affecting the ability to achieve a successful scale of operation
- Significant cost of electronic health records (EHRs) and data submissions, as well as difficulties in implementing EHR systems
- Increase in regulatory costs
- High infrastructure costs
Strategies to increase financial viability for hospice providers can include:
- Becoming a nonprofit 501(c)(3) organization, which allows the hospice to accept donations, major gifts, bequests, and planned giving
- Offering home and outpatient services in residences or home-like settings
- Holding community fundraisers throughout the year
- Charging a room and board rate for care in a hospice home at the routine level
- Offering all 4 levels of hospice care: routine home care, general inpatient care, continuous home care, and inpatient respite care
- Enrolling patients early in their diagnosis
- Leveraging telehealth (virtual and telephonic) visits to supplement in-person visits
What strategies can help make a rural palliative care service financially viable?
Sustainability Strategies for Community-based Palliative Care, a summary of two roundtable discussions conducted by Stratis Health in 2018 with 9 rural palliative care programs, highlights that in addition to Medicare and other payers not having a distinct palliative care benefit, only some members of a palliative care team can bill for direct services. This document also offers examples and resources to support rural community-based palliative care programs including traditional billing and reimbursement, grants and philanthropy, value-based contracting, and emerging opportunities such as the development of a palliative care benefit other new payment models for rural healthcare providers. The National Academy for State Health Policy has also compiled several reimbursement strategies for state health programs to implement to promote sustainable palliative care services for Medicaid beneficiaries.
How do rural hospice providers compare on quality of care and patient satisfaction measures?
According to the 2015 article Quality of Hospice Care: Comparison Between Rural and Urban Residents, rural hospice patients and their families were more likely than their urban counterparts to report high levels of satisfaction with overall care and pain and symptom management. Of the 331 rural people surveyed, only 3 patients were not satisfied with the hospice care they received. The researchers suggested that the high ratings for rural hospices may be due to:
- Rural communities' connectedness
- Services being delivered quickly, as providers know the patients' needs
- Highly individualized care, provided by nurses who ensure that patients receive excellent service
- Neighbors who are aware of patients' needs and are willing to help
Medicare.gov's Care Compare tool allows users to find and compare hospice agencies in their area in terms of the quality of patient care and caregiver experience compared to national averages.