Jul 28, 2021
Federal Agencies' Investment in Rural Cancer Control Fosters Partnerships between Researchers and Rural Communities
by Mary Charlton, PhD; Whitney Zahnd, PhD; Jennifer Patterson, MPH, Kimberly Merchant, MA
 As a young girl,
Stephanie Wheeler, PhD, MPH, spent much of her youth
on her grandparents' farm in rural South Carolina. Her
early experiences with healthcare were colored by
witnessing family members navigate a number of obstacles:
delays in care, lack of health insurance, shortage of
providers, and mistrust in the healthcare system. When
her uncle, a self-employed farmer with no health
insurance, later experienced symptoms consistent with a
brain tumor, he faced barriers in getting diagnostic
testing and in finding hospitals that would provide cost
estimates for his treatment or treat him without
insurance. Once he finally had surgery to remove the
tumor, he was billed over $100,000, which was turned over
to debt collectors who harassed him for payment on an
ongoing basis. Fortunately, the hospital eventually
agreed to forgive his debt as charity care, but not
without considerable anxiety and distress as he, Wheeler,
and other family members attempted to deal with the cost
of his care, including applying for — and being
denied — Social Security disability and
Medicaid insurance.
As a young girl,
Stephanie Wheeler, PhD, MPH, spent much of her youth
on her grandparents' farm in rural South Carolina. Her
early experiences with healthcare were colored by
witnessing family members navigate a number of obstacles:
delays in care, lack of health insurance, shortage of
providers, and mistrust in the healthcare system. When
her uncle, a self-employed farmer with no health
insurance, later experienced symptoms consistent with a
brain tumor, he faced barriers in getting diagnostic
testing and in finding hospitals that would provide cost
estimates for his treatment or treat him without
insurance. Once he finally had surgery to remove the
tumor, he was billed over $100,000, which was turned over
to debt collectors who harassed him for payment on an
ongoing basis. Fortunately, the hospital eventually
agreed to forgive his debt as charity care, but not
without considerable anxiety and distress as he, Wheeler,
and other family members attempted to deal with the cost
of his care, including applying for — and being
denied — Social Security disability and
Medicaid insurance.

Wheeler currently serves as the Associate Director of Community Outreach and Engagement at the University of North Carolina Lineberger Cancer Center and as Principal Investigator of the Coordinating Center for the Cancer Prevention and Control Research Network. Her uncle's experience motivated some of her research on addressing financial barriers to care. She received a grant from the National Cancer Institute to study the implementation of financial navigation services in rural oncology practices, in which she partners with rural clinics to train and support a team of financial navigators to identify financial support resources, clarify cost expectations, and develop strategies to cope with high costs of care.
Based on her personal and professional experiences, Wheeler summarized some of the issues that contribute to a greater financial burden to cancer patients living in rural communities: “[Rural patients] often have smaller social networks with insufficient capital on which they can rely when catastrophic medical expenses occur, fewer local resources such as nonprofits and cost assistance organizations, and they are often employed by smaller employers that can't afford comprehensive and generous insurance plans, and many are self-employed so purchasing insurance on their own can be cost-prohibitive.”
Like many researchers, Wheeler's life experiences laid the foundation for cancer research projects that came to life in part due to funding from federal agencies such as the National Cancer Institute (NCI), Centers for Disease Control and Prevention (CDC), and the Health Resources and Services Administration (HRSA). Such federal funding has enabled many innovative projects and has helped build and strengthen relationships between rural partners and researchers at large academic centers.
Federal Agencies Partner to Promote Rural-Focused Cancer Research
The NCI advocated for further investment into research on rural cancer disparities after finding that only 3% of NCI-funded research grants were focused on rural cancer control issues. As part of new rural-focused funding opportunities, it awarded supplemental grants to 27 NCI-designated cancer centers across the U.S. in 2018 and 2019. These grants required researchers to work directly with rural providers, organizations, and community members to address rural cancer control issues present in their community. Additional grant opportunities have become available to researchers regardless of cancer center affiliation to help address rural cancer disparities.
Coming Together Around Rural Cancer Prevention and Control
NCI partnered with other federal agencies including CDC, HRSA's Federal Office of Rural Health Policy, and the Centers for Medicare and Medicaid Services' Rural Health Council, to host the “Accelerating Rural Cancer Control Research” meeting in 2018. There, over 250 researchers, medical and public health practitioners, and representatives of community organizations worked to identify gaps in the research, build partnerships to address challenges in rural cancer prevention and control, and develop recommendations to accelerate rural cancer control.
Rural cancer control has also become an increasing
priority of the Cancer Prevention and Control Research
Network (CPCRN), a CDC- and NCI-funded network of
academic, public health, and community partners across
the country who collaborate to reduce cancer disparities.
In 2018, the Network launched a Rural Cancer
Workgroup, composed of faculty, staff, and students
from CPCRN centers and affiliates as well as CDC and NCI
staff, which is focused on addressing challenges
experienced by rural populations, rural cancer patients
and survivors, and rural providers. Dr. Wheeler
believes CPCRN's commitment to serving rural patients
makes it unique from larger cancer control programs:
“It helps to broaden the lens to think about
the real-world experience of patients who are outside of
major urban hubs and living farther from large academic
centers.”

Shobha Srinivasan, PhD, and Amy Kennedy, PhD, MPH, both in the NCI Office of the Director, Division of Cancer Control and Population Sciences, are among those who oversee the rural cancer-focused grant funding. They have facilitated collaboration and networking among grant recipients so that lessons learned in building rural cancer control research capacity can be shared across the U.S. Srinivasan recounted the goal of the rural-specific funding: “We are seeing cancer rates increasing in rural areas…What NCI has made very clear is that we need to look at what we aren't doing well in rural areas and address those challenges in a responsive manner.”

Srinivasan feels there has been a great deal of support within NCI and coordination across federal agencies. She points out the value of partnering with other agencies such as HRSA, CDC, and the U.S. Department of Agriculture, which has been integral to building this agenda and sustaining it. For example, NCI used screening programs implemented by CDC in rural areas as models, building on them to also include follow-up care and survivorship components.
Kennedy gets her drive and commitment to rural health from observing the range of projects that they fund: “I like seeing the varied activities that we are funding, from prevention work to interventions, to access to care. There are so many different angles to tackle rural cancer control issues; there is always more work to be done.”

Dr. Lisa Richardson, Director of the Division of Cancer Prevention and Control, is the lead for rural cancer activities at CDC. She said, “Data provide the foundation for the work being done to reduce the cancer burden gap between rural and urban Americans.” Cancer incidence data are available from CDC's National Program of Cancer Registries and NCI's Surveillance, Epidemiology, and End Results, and cancer death data are accessible from CDC's National Vital Statistics System. Using these data, CDC produced the first report to detail cancer differences and mortality gaps between rural and urban areas.
Partnerships are key to reducing cancer incidence and the associated disparities in rural communities.
“We can address urban/rural cancer disparities through targeted public health efforts in collaboration with our cancer control stakeholders. Partnerships are key to reducing cancer incidence and the associated disparities in rural communities,” Richardson said.
CDC's National Comprehensive Cancer Control Program (NCCCP) has provided funding, guidance, and technical assistance to help states, territories, and tribal organizations to design and implement impactful, strategic, and sustainable plans to prevent and control cancer. The CDC-funded Cancer Prevention and Control Research Network (CPCRN) is working to evaluate how these interventions impact rural communities in their cancer control plans. The division is also funding a project that aims to increase the quality of cancer survivor care in rural communities through reducing disparities in patient navigation and tele-mentoring.
“Engaging patient navigators can help increase the effectiveness of communication between healthcare specialists and other healthcare providers,” explained Richardson. “Also, tele-mentoring can increase the knowledge and skills of multidisciplinary healthcare provider teams to help reduce high-risk health behaviors, improve cancer screening, and increase HPV vaccination uptake among cancer survivors.”
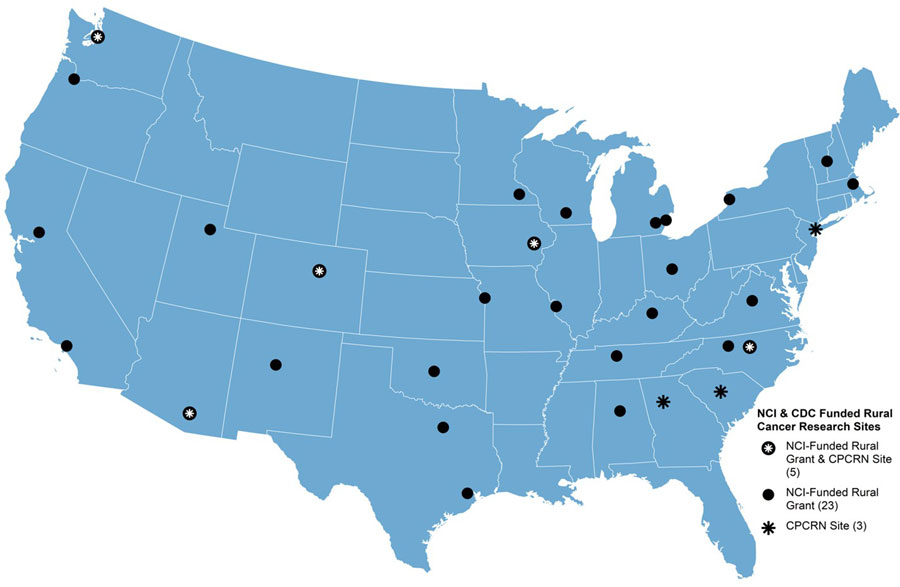
With a focus on rural cancer control, these funding opportunities have brought more attention to rural areas of the country that experience particularly high burdens of cancer and cancer deaths. Federal funding has allowed researchers who are committed to rural health issues to broaden the reach and scope of their projects. It has also attracted cancer researchers from different backgrounds to expand their work into addressing rural disparities. Funding has facilitated research partnerships with rural communities and providers striving to overcome resource constraints to deliver comprehensive cancer prevention and control services to their patients. In part due to this funding, many successful partnerships have been established throughout the country. The map below illustrates the locations of different sites across the U.S. that have received rural cancer-focused funding from the NCI and those participating in the CPCRN. Examples of successful partnerships between researchers and rural community members and providers to enhance rural cancer prevention and control are described below.
Increasing Participation in Clinical Trials for Cancer Prevention and Control

Jackilen Shannon, PhD, Associate Director of Oregon Health & Science University's Knight Cancer Institute's Community Outreach and Engagement program, and Paige Farris, MSW, Community Research Project Director, work with rural primary care provider and oncology research teams to increase the readiness of patients to participate in cancer prevention trials. Farris, who has lived most of her life in rural towns, explained the goal of this work.

“Large urban cancer centers typically say, 'We want everyone in clinical trials!' But we are working with very small, under-resourced providers, and they don't have the capacity to run those types of complex clinical trials focused on cancer treatment. So we are thinking through the feasibility of implementing cancer prevention trials — including interventions related to physical activity, healthy eating, HPV vaccinations — aligned with other chronic disease prevention, which help rural hospitals meet the standards for Commission on Cancer accreditation while also making their rural communities healthier.”
Shannon indicated that local clinics are using clinical case managers as patient care supporters and have identified unique community linkages and champions supportive of cancer prevention and control efforts as well as leaders of large regional health systems.
Developing Human Papillomavirus (HPV) Vaccination Intervention Strategies to Improve HPV Vaccination Rates

Huntsman Cancer Institute is the only NCI-Designated Cancer Center in the five-state Mountain West region (Utah, Nevada, Wyoming, Montana, and Idaho), which is largely rural and frontier. Deanna Kepka, PhD, MPH, is an Associate Professor at the University of Utah and a member of the Huntsman Cancer Institute's Cancer Control and Population Sciences program. Kepka's research focuses on increasing HPV vaccination rates, as the Mountain West region has some of the lowest vaccination rates in the country. She and her team surveyed pediatric healthcare providers and clinic staff, who have opportunities to influence individual HPV vaccination decisions, about HPV vaccination knowledge and recommended practices.
Kepka reported that “responses to our survey indicated that lack of reminders, vaccine hesitancy, and the cost of the vaccine were the primary obstacles to vaccination. Based on these results, we developed and tested the use of an HPV vaccination text message as a reminder for patients.”
They also recently fielded a survey that was completed by more than 1,400 rural 18- to 26-year-olds living in 12 western U.S. states with an oversampling of rural residents. They found that rural residents had a lower HPV vaccination rate (any doses) than did urban residents (38% versus 48%, respectively).
Findings are being synthesized and an implementation plan will be developed in partnership with clinics serving rural patients for an HPV vaccination catch-up program.
HPV Vaccine Research in Georgia
The Emory CPCRN team, led by Dr. Cam Escoffery, is conducting research to promote HPV vaccination in rural counties in southwest Georgia. The team is conducting telephone interviews with parents, their teen(s)/adolescent(s), and young adults on HPV vaccine knowledge, attitudes about the vaccine, intentions to get vaccinated, and facilitators and barriers to getting the vaccine. Public health professionals and healthcare providers are also being interviewed about barriers and facilitators to vaccine uptake among their patients and/or community.

Natoshia Askelson, PhD, is co-lead of Community Outreach and Engagement at the University of Iowa Holden Comprehensive Cancer Center and co-lead of the CPCRN Rural Workgroup. Her interest in HPV vaccination in rural areas has been driven by the geography of Iowa, where vaccination rates tend to be much lower in rural counties. Because most HPV interventions are not implemented in rural areas, her team is studying how best to adapt them to these communities and provide support for rural clinics. The first step is to use a concept mapping approach to generate feedback on implementation challenges among stakeholders in five rural states: Iowa, Minnesota, South Dakota, Oregon, and Washington. Concept mapping is a strategic planning tool that enables stakeholders to visually organize ideas to guide public health planning. These findings support using a multilevel intervention approach that addresses individual, interpersonal, organizational, community, and policy levels to improve HPV vaccination.
Askelson is particularly excited about how federal funding has allowed her team to leverage their expertise to serve their community partners and help them execute their cancer control ideas and projects. She recounted how their team was able to support the work of one nurse practitioner working on HPV in rural health clinics: “We were able to pull together the team to provide targeted support pretty quickly…which I think would be really hard for a rural clinic to do without partners like us…it also elevates her leadership at her own clinic.”
Increasing Colorectal Cancer Screening Rates in Rural Communities

Some cancer researchers have specifically focused on rural areas of the U.S. that are known to be cancer hotspots. For example, the lower Mississippi Delta has the highest rate of colorectal cancer (CRC) deaths in the country. Since the Delta region includes counties in Missouri and Illinois, Bettina Drake, PhD, MPH, Professor of Surgery at the Washington University School of Medicine and Associate Director of Community Outreach and Engagement at Siteman Cancer Center in St. Louis, is working to build research capacity among community healthcare and public health organizations in rural Illinois. Their Community Outreach and Engagement team, along with research coordinator Nora Leahy, partnered with six southern Illinois community stakeholders with diverse professional backgrounds to adapt a community research training program tailored to healthcare providers. The team then worked with some of the stakeholders, including the American Cancer Society of Central and Southern Illinois, to implement a pilot project to provide education on colorectal cancer screening to providers in a large regional hospital and clinic system. The pilot project objectives were to improve rates of colorectal cancer screening, including all recommended screening options, through increasing provider confidence, awareness of, and intent to recommend evidence-based colorectal cancer screening practices. While results showed increased awareness of screening options among providers, the COVID-19 pandemic introduced system- and patient-level barriers to screening.
Pharmacy-Based Screening
The University of North Carolina CPCRN is developing PharmFIT, an innovative pharmacy-based program for increasing access to CRC screening. The program distributes FIT (fecal immunochemical test) kits, which can be used to screen for CRC, through community-based pharmacies. The kit can be completed at home and mailed to a community lab for processing.
According to Dr. Alison Brenner, one of the principal investigators of this study, PharmFIT shows promise in addressing CRC obstacles: “When we interviewed patients, they seemed very receptive to obtaining a simple cancer screening test from their local pharmacy,” she said. “Likewise, pharmacists were generally very open to the idea of offering FIT kits as they already provide flu shots and other types of preventive services.”
Leahy, whose previous projects focused on racial/ethnic
disparities in cancer, reported that rural cancer
disparities research was new to her but noted,
“Once I started working in rural disparities, I
realized that we are dealing with the same barriers and
challenges [as in racial/ethnic disparities] that just
look a little different.”

The Central Appalachian region is another major hotspot for CRC deaths. Jamie Zoellner, PhD, RD, Associate Director of the University of Virginia Cancer Center Without Walls, formed a multi-disciplinary Cancer Control Leadership Team with members from the University of Virginia Cancer Center and Stone Mountain Health Systems (SMHS), an 11-clinic Federally Qualified Health Center (FQHC) located across seven rural counties in southwest Virginia. Throughout the 11 SMHS clinics, electronic medical record data showed CRC screening rates of age-eligible patients (50-75 years) at 30% in 2018, which was well below the national average of 69% and the national goal of 80%.
Staff and patients were interviewed to identify barriers and opportunities to improve CRC screening within SMHS. According to staff, factors within SMHS clinics that helped promote CRC screening included high workplace satisfaction, experiences with tracking other types of cancer screenings, and a highly active Performance Improvement Committee. The organization's efforts were hindered by electronic medical record inefficiencies and requiring patients to physically return fecal tests to the clinic. Patient barriers to CRC screening included cost, fear, transportation, and lack of motivation due to not having any symptoms of CRC.
According to Zoellner, “Collaborative research and quality improvement efforts are currently underway to build on these findings to roll out CRC-related initiatives aimed at applying evidence-based strategies to increase CRC screening at SMHS.”

Jan Eberth, PhD, Director of the Rural and Minority Health Research Center at the University of South Carolina Arnold School of Public Health and co-founder and co-lead of the Rural Workgroup in the Cancer Prevention and Control Research Network, is currently engaged in studies examining cancer screening accessibility and its impact on patient-level outcomes like stage at cancer diagnosis and survival. With funding from HRSA, NCI, and the American Cancer Society, Eberth has examined the intersection of race/ethnicity and rurality in colorectal and cervical cancer disparities. She is currently piloting evidence-based interventions to increase colorectal cancer screening in Rural Health Clinics and has explored trends in spatial access to colonoscopy in South Carolina.
Implementing Recommendations
The National Advisory Committee on Rural Health and Human Services released recommendations for rural cancer prevention and control efforts in the fall of 2019. One recommendation was related to the consideration of rural cancer mortality disparities in comprehensive cancer control plans. Thus, since 2020, the CPCRN Rural Cancer Workgroup has been focused on assessing how states, territories, and tribal organizations address rural in their comprehensive cancer control plans' processes, data, goals, objectives, and strategies. This is being accomplished by 1) completing a content analysis of current plans and 2) conducting interviews with comprehensive cancer program directors throughout the country to see how they are engaging rural stakeholders in their cancer control planning.
Although her career began with a focus on racial/ethnic
disparities more generally, an interest in health
geography led her to develop a research program
reflecting the intersection of race/ethnicity, rurality,
and healthcare accessibility. Eberth discussed the
progress that has been made in rural cancer research,
which ultimately led to more funding from federal
entities and rural-relevant data and resources:
“That didn't happen overnight. It happened
because of key
landmark studies…and the dogged advocacy of people
like my mentor,
Jan Probst, who kept knocking on doors and saying,
'We need more access to urban/rural indicators in public
use data!' Those two things together were probably what
got us to the place we are now.”
Connecting with Key Stakeholders to Address Health Behaviors and Prevent Cancer

Robin Vanderpool, DrPH, is chief of the Health Communication and Informatics Research Branch (HCIRB) in the Division of Cancer Control and Population Sciences at NCI. Vanderpool is a part of the CPCRN rural cancer workgroup and has done extensive community-based research in rural Kentucky in her previous role with the University of Kentucky's Markey Comprehensive Cancer Center. Vanderpool noted that obtaining buy-in and support from local community groups — and engaging them as collaborators — is a critical component needed to impact cancer control in the long term: “It's about showing that you're there for the long haul and you want to give back to the community.”
She said the way to be successful is to concentrate on social determinants of health, through considering “the environment in which people live and work and try to be healthy…we've got to be more multi-level and contextual in approaches…if you don't use a multi-level approach, it won't be sustainable to reach longer-term goals.”
We are not going to take something that worked elsewhere in an urban area and just plunk it into a rural area. What we are trying to do is understand what is happening within the rural context/framework, understand their needs, and adjust — meeting people where they are.
Similarly, Srinivasan noted the importance of recognizing that the unique characteristics of each community dictate the approach or intervention. She said, “We are not going to take something that worked elsewhere in an urban area and just plunk it into a rural area. What we are trying to do is understand what is happening within the rural context/framework, understand their needs, and adjust — meeting people where they are.” Federal funding has made it possible to engage rural regions in research that will benefit their communities, allowing those working and living in rural areas to inform the research. Kennedy cites this as a crucial element to the funding NCI provides: “Having investigators at cancer centers or researcher-intensive universities partner with local-level hospitals and community groups is critical. These partnerships build trust and promote participation in the research.” She added that the key in gaining trust from local communities is the promise that cancer prevention and control interventions are going to be long-term investments, something NCI emphasizes in the funding opportunities: “Sustainability is key to truly impacting the community in a positive way.”
In addition to the aforementioned projects addressing specific cancer types or preventive approaches, some CPCRN sites are demonstrating the important community connections that Vanderpool, Srinivasan, and Kennedy note to address broader cancer challenges. The University of Arizona CPCRN team members have been able to form meaningful connections with cancer survivors of Mexican origin living on the southern Arizona border. They have accomplished this by having bicultural and bilingual staff — who understand the culture and traditions that influence lifestyle choices and behaviors — interact with cancer survivors and their caregivers. Further, the team was able to learn about the community-wide perspectives and beliefs about healthy lifestyle behaviors, challenges, and cancer survivorship to enhance the planning for future programs in this area.

The South Carolina CPCRN (SC-CPCRN) supports community organizations' cancer prevention and control efforts as part of its Community Health Intervention Program. Dr. Daniela Friedman, principal investigator, described the work of this year's grantees: “They will focus on physical activity to combat cancer in rural communities and lead a cancer screening initiative encouraging preventive care in rural areas that may have been delayed due to COVID-19.” The SC-CPCRN's work is guided by a Community Advisory Council of individuals representing rural health, primary care, and faith-based and other organizations.
The success of these federally funded opportunities illustrates the dedication of researchers, practitioners, and communities who are making efforts to expand access, promote prevention, and improve treatment of cancer in rural communities across the country. Rural partners are critical to guide research consistent with the needs and priorities of the communities they serve. While there are unique challenges to providing cancer prevention and control services in rural settings, there are also strengths and advantages in rural communities to learn from and build into future research endeavors. For example, Wheeler found that while rural areas may have fewer financial resources to assist cancer patients, the smaller size of rural centers can make the financial navigation process much more straightforward and accessible compared to large urban/academic settings: “The overall patient experience in terms of navigating the system is probably better because of the close-knit nature of these communities and the support staff who are serving them. Everybody knows everybody; there's more familiarity.”
To maintain and expand the academic-rural partnerships that have been developed in recent years, continued funding support focused on rural cancer prevention and control is critical to advance research and reduce cancer burden in rural areas. Eberth acknowledges that the funding offered to date has helped “to jump-start rural partnerships and to elevate the priority of cancer prevention and control initiatives in rural areas, but continued support is imperative to keep the momentum going.” Nearly all the featured researchers expressed that continued collaboration and coordination of rural-focused funding that includes more multi-year grant opportunities are key to accelerating partnerships and progress in reducing the burden of cancer in rural areas.